352.204.0094
[gtranslate]

Choosing the most effective metabolic solution feels confusing because the options — Semaglutide and Tirzepatide — seem so similar on the surface.
Put simply: Tirzepatide is a dual-action compound that generally produces greater average weight loss (up to 22.5%) and A1C reduction than single-action Semaglutide (up to 17%).
However, both are best-in-class tools for profound metabolic improvement.
You need to know exactly how the dual-action science works, which compound’s data better matches your personal goals, and how a tailored protocol gets you back to walking with your neighbor or enjoying stress-free weekend BBQs.
Here is how tirzepatide and semaglutide actually differ in mechanism, results, risks, and ideal patient fit — so you can match the right level of clinical firepower to your real‑world goals.
TL;DR: Tirzepatide is Stronger, But Semaglutide May Be the Better Fit
- Tirzepatide is your higher-ceiling option. The dual GIP/GLP-1 action consistently delivers greater average weight loss (up to 22.5%) and larger shifts in A1c and metabolic risk markers than single-action Semaglutide.
- Semaglutide remains a best-in-class tool for strong, steady weight loss (up to 17%), boasts the longest track record of safety data, and has proven cardiovascular event reduction in high-risk patients.
- The choice hinges on your risk profile: Tirzepatide is the better fit for severe obesity, stacked risks (MASLD, OSA, high CV burden), or when you need maximum, rapid weight loss. Semaglutide suits moderate risk and patients prioritizing tolerability and established evidence.
- The “better” drug is the one that aligns with your lab data, side-effect tolerance, budget, and long-term goals. Use your data to track, talk with your provider, and tweak the protocol for your unique metabolism.

What Are They? Tirzepatide vs Semaglutide
Tirzepatide and Semaglutide are the two leading injectables in the incretin class, moving past basic blood sugar maintenance to deliver the most profound, non-surgical body composition resets available to clients today.
What is Tirzepatide?
Tirzepatide (Zepbound, Mounjaro) provides the higher ceiling of metabolic optimization because it leverages two distinct hormone pathways in a single, once-weekly injection.
Tirzepatide is the first-in-class dual GIP and GLP-1 receptor agonist. This means the compound hits two receptors simultaneously, maximizing appetite suppression and fat metabolism where the single GLP-1 signal can eventually face resistance or regulatory limits and fall short.
- Your Protocol: Clients receive the solution once weekly via a convenient, pre-filled subcutaneous auto-injector.
- Status: The FDA approves the compound (as Zepbound) for chronic weight management and (as Mounjaro) for Type 2 Diabetes.
Tirzepatide is your dual-action command.
What is Semaglutide?
Semaglutide (Wegovy, Ozempic, Rybelsus) laid the indispensable groundwork for this revolution, operating as a proven, highly effective single-action GLP-1 receptor agonist delivered weekly or daily.
Semaglutide is a potent mimetic of the GLP-1 hormone, the established signal that slows digestion and sends satiety cues directly to the brain. It is the gold-standard protocol for robust appetite control.
- Your Options: Clients primarily use the simple, once-weekly injection, though a daily oral tablet option (Rybelsus) also exists for a customized protocol approach.
- Status: The FDA approves the compound (as Wegovy) for chronic weight management and (as Ozempic/Rybelsus) for Type 2 Diabetes.
Semaglutide is your single-action foundation.
How Do They Work? Tirzepatide vs Semaglutide
Semaglutide uses a single tool (GLP-1) to regulate your appetite, while Tirzepatide uses a dual tool (GLP-1/GIP) to execute a more aggressive, systemic metabolic takeover.
Both medications turn down appetite and stabilize blood sugar, but they do it with different “hormone blueprints,” which is why they land differently in real life.
What is the Difference Between the GLP-1 and Dual GIP/GLP-1 Signals?
The mechanism determines the scope of the metabolic repair. Both solutions tackle hormonal signaling, but their depth of reach differs.
- GLP-1 (Semaglutide’s Core Function): This established pathway mimics the hormone that slows the movement of food out of the stomach and triggers satiety signals to the brain. This is the primary, proven brake on appetite and blood sugar spikes, forming the essential foundation of modern metabolic optimization.
- GIP’s Added Role (Tirzepatide’s Dual Function): The GIP action is Tirzepatide’s key distinction. It complements the appetite control of GLP-1 while also directly impacting fat cells (adipocytes) and enhancing insulin sensitivity in a unique way. This dual-signal approach overcomes the potential resistance or ceiling that the single GLP-1 pathway can eventually reach.
What this means for your day‑to‑day
- Semaglutide sends a single GLP‑1 signal that slows stomach emptying, improves post‑meal insulin response, and tells your brain “you have had enough,” which usually shows up as fewer cravings and smaller meals feeling satisfying.
- Tirzepatide layers GIP on top of GLP‑1, so you see similar appetite and gastric‑emptying effects plus extra help with insulin and lipid handling, which often translates into a deeper drop in hunger and faster, larger changes on the scale and in labs.
Why the mechanism should guide the choice
- For someone with severe obesity or stacked cardiometabolic risk, tirzepatide’s dual‑signal intensity can be an advantage — if they are ready for tighter titration, closer follow‑up, and stricter nutrition to protect lean mass and minimize GI symptoms.
- For someone aiming for strong but steady weight loss with a focus on tolerability and habit‑building, semaglutide’s single‑pathway action can be the better match, giving real movement in weight and A1c without feeling like the appetite dial is turned all the way down.

How Does Tirzepatide vs. Semaglutide Compare for Weight Loss?
Tirzepatide generally delivers more weight loss than semaglutide, but both sit in a different league from older medications and lifestyle‑only care. Those percentages only matter if they change how your body actually moves, sleeps, and survives — how hard your joints work, how deeply you rest, and how soon big diagnoses or surgeries stop looming on the calendar.
What the Trials Show: Tirzepatide vs. Semaglutide
- In the SURMOUNT‑1 trial, adults with obesity but no diabetes lost about 16%, 21%, and 22.5% of their starting weight on tirzepatide 5 mg, 10 mg, and 15 mg once weekly, with average losses at the top dose around 52 pounds.
- In the STEP 1 trial semaglutide obesity trials, once‑weekly semaglutide 2.4 mg produced roughly 15% average weight loss at 68 weeks, far outperforming placebo and older agents.
- A 2025 meta‑analysis pooling randomized trials and real‑world cohorts found tirzepatide produced about 4 percentage points more weight loss than semaglutide overall, with a clear dose‑response when tirzepatide doses exceeded 10 mg.
- Recent head‑to‑head and cohort work in adults with overweight or obesity confirms this pattern: tirzepatide is consistently superior for absolute weight and waist‑circumference reduction at roughly 72 weeks.
What do those percentages mean in real life?
For a 250‑pound patient:
- a 15% loss on semaglutide is roughly 37–38 pounds
- a 22.5% loss on high‑dose tirzepatide is about 56 pounds — an extra 18–20 pounds off the joints and out of visceral fat stores.
In SURMOUNT‑1, quality‑of‑life analyses linked tirzepatide‑driven weight loss to better physical functioning, less pain, and improved daily activities — the difference between avoiding stairs and climbing them without bargaining with your knees.
Tirzepatide body‑composition data show most of the lost weight is fat mass, which matters for mobility, sleep apnea, and cardiometabolic risk; semaglutide shows similar preferential fat loss but with a somewhat smaller overall magnitude.
Verdict: Who actually needs maximum weight loss?
Some bodies truly need the extra push that tirzepatide offers. But others do better with semaglutide’s steadier curve.
When tirzepatide’s “extra” makes clinical sense:
- Severe obesity with stacked risks (BMI over 30, diabetes, hypertension, MASLD, sleep apnea, etc.)
- High orthopedic burden (advanced knee or hip arthritis, foot/ankle issues)
- Pre‑surgical timelines (preparing for bariatric, orthopedic, or heart surgeries)
When semaglutide may be the better fit:
- Mild to moderate obesity with lower short‑term risk.
- Patients with fragile nutrition, eating‑disorder history, or concern about overly aggressive appetite suppression.
- Anyone prioritizing steady, sustainable loss and habit change over maximum speed, while still wanting enough movement to change labs, joint load, and daily energy.
How Do Tirzepatide and Semaglutide Affect Heart and Metabolic Risk?
Both drugs clean up cardiometabolic risk. Tirzepatide just tends to push harder on multiple levers, while semaglutide brings the longer track record and rock‑solid proof in higher‑risk patients.
How Tirzepatide vs Semaglutide Move the Risk Markers
Both tirzepatide and semaglutide reliably lower:
- A1c and fasting glucose
- Blood pressure
- Waist size and visceral fat
- “Bad” lipids like non‑HDL and triglycerides
- Overall calculated 10‑year cardiovascular risk
But tirzepatide usually moves those numbers farther and faster. In risk‑modeling work, it cut 10‑year CV risk by roughly 2.4% absolute, compared with about 1.4% for semaglutide, mainly because it drops BMI and systolic blood pressure more.
Semaglutide, however, already has SELECT‑level proof that in people with obesity and existing cardiovascular disease (but no diabetes), it reduces major heart events by about 20% versus placebo — evidence tirzepatide is still catching up to in non‑diabetes populations.
Verdict: Who Should Get Which for Heart and Metabolic Risk?
- Tirzepatide is the better fit when risk is stacked: significant obesity plus diabetes, MASLD, sleep apnea, or multiple cardiovascular risk factors, where the priority is maximum multi‑marker change in the shortest safe window.
- Semaglutide is the better fit when risk is moderate or the patient (or insurer) wants the longest, clearest outcome data: obesity with earlier‑stage cardiometabolic disease, where strong improvements and proven event reduction are enough without deploying dual‑agonist intensity.
How Do Tirzepatide and Semaglutide Support Liver and Sleep Health?
Both drugs pull fat out of the liver and pressure off the airway, but tirzepatide usually hits harder, while semaglutide brings more mature liver data today.
How Tirzepatide vs Semaglutide Help the Liver
MASLD (what used to be “fatty liver”) is excess fat and inflammation in the liver driven by insulin resistance, visceral fat, and metabolic overload; left alone, it can progress to MASH, fibrosis, and cirrhosis.
- Tirzepatide trials in MASLD/MASH show meaningful drops in liver fat, liver enzymes, and inflammatory changes on biopsy, with higher rates of NASH/MASH resolution and fibrosis improvement compared with placebo.
- Semaglutide also improves MASLD and MASH: phase 2 and phase 3 work, plus large real‑world cohorts, link it to better liver histology, less fibrosis progression, and improved survival in MASLD patients versus controls.
Both drugs are legitimate liver‑protection tools in metabolic disease.
Tirzepatide appears to deliver a stronger, multi‑hormone push on liver fat and inflammation, while semaglutide currently has broader, longer real‑world outcome data in MASLD.
How Tirzepatide vs Semaglutide Help Sleep Apnea
Obstructive sleep apnea (OSA) is often a weight‑around‑the‑neck and visceral‑fat problem. Weight loss alone can reduce apnea — hypopnea events and nighttime oxygen drops.
- Tirzepatide (Zepbound) is now FDA‑approved specifically to treat OSA in adults with obesity, backed by SURMOUNT‑OSA trials showing large drops in apnea–hypopnea index, hypoxic burden, and body weight versus placebo.
- Semaglutide is not OSA‑approved but still improves apnea severity in some patients as weight and visceral fat come down, with emerging data suggesting symptom relief and better functional scores.
For sleep apnea driven by obesity, both agents can help, but tirzepatide is the one positioned as a direct OSA drug today. It’s the stronger and your only FDA-approved choice when apnea is a central problem.
Verdict: Who Wins for Liver and Sleep Health?
Cleaner liver labs and imaging plus deeper, less fragmented sleep translate into better daytime energy, clearer thinking, more stable mood, and lower long‑term risk of cardiovascular and liver events.
Tirzepatide suits patients who need to hit liver disease or moderate‑to‑severe sleep apnea hard — people where every extra notch of weight and visceral‑fat reduction matters for keeping them out of future procedures and hospital rooms.
Semaglutide fits patients who want dependable, steady improvement in liver health and snoring or mild‑to‑moderate apnea symptoms, but do not need or want the most aggressive weight‑loss engine just to sleep better and clean up their labs.
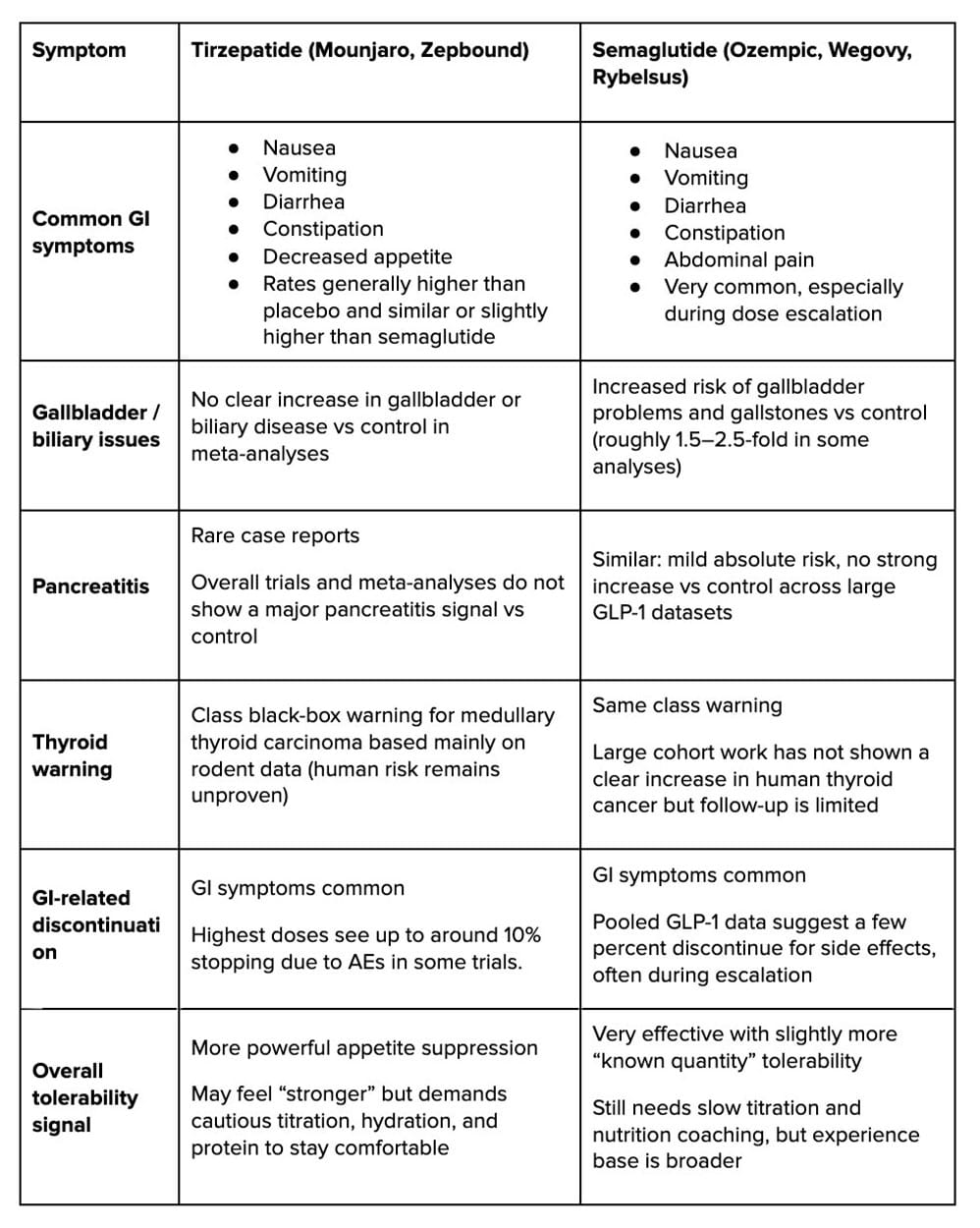
What Side Effects and Risks Should You Expect?
Both tirzepatide and semaglutide cause the familiar GLP‑1‑style side effects — mainly gut upset and rare gallbladder or pancreas issues — but tirzepatide tends to feel stronger on appetite and GI intensity, while semaglutide carries a slightly higher gallbladder signal and the longer real‑world safety track record.

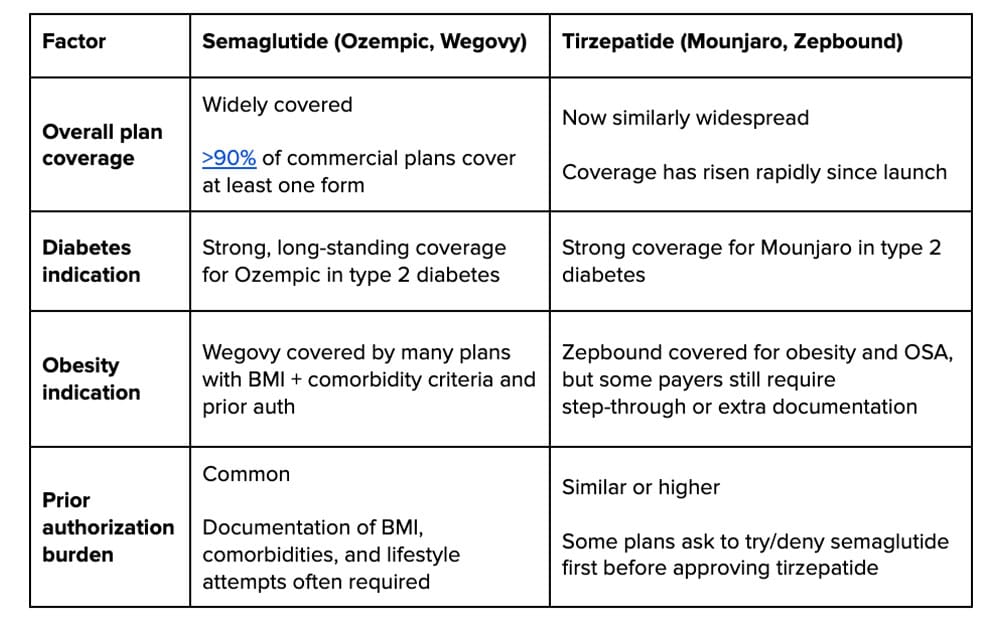
How Do Cost, Coverage, and Access Differ?
When a plan covers anti‑obesity meds, out‑of‑pocket costs for the two are usually in the same ballpark. But when it doesn’t, both are essentially unaffordable unless a manufacturer savings card applies. And those cards are temporary, rule‑heavy, and can disappear or tighten at any time, so no “cheaper” label is guaranteed long term.
Insurance coverage at a glance
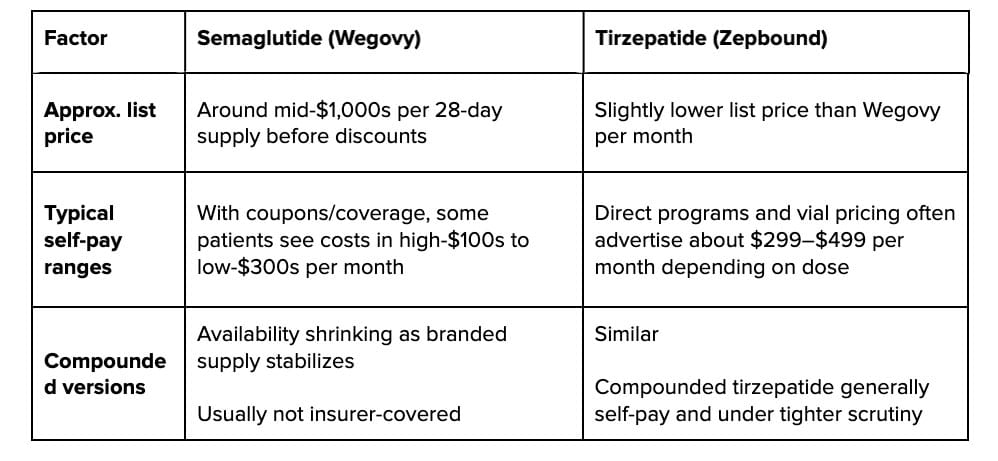
Cash‑pay realities
Who Is a Better Fit for Tirzepatide vs Semaglutide?
Tirzepatide is the higher‑intensity tool. Semaglutide is the steadier backbone. The better fit depends on how much risk you are carrying and how aggressively you want to move weight, labs, and symptoms.
Who leans toward tirzepatide?
- Severe or multi‑system metabolic disease: Significant obesity plus diabetes, MASLD, OSA, or clustered cardiovascular risk factors, where every extra few percentage points of weight and risk reduction matter.
- Patients who need maximum, not moderate, change: Those aiming for 20%‑plus loss to qualify for surgery, offload joints, or defuse high‑stakes diagnoses in a defined time window.
- Patients who can handle tighter structure: People willing to tolerate stronger appetite suppression, closer titration, and more lab and nutrition oversight in exchange for bigger, faster shifts in body weight and cardiometabolic markers.
Who leans toward semaglutide?
- Mild to moderate obesity or earlier‑stage risk: Patients who need strong but not maximal weight loss and already have improving labs with GLP‑1–level therapy.
- Patients prioritizing tolerability and evidence comfort: Those who want a powerful, predictable medication with the longest real‑world CV and liver outcomes data and are wary of “turning the dial all the way down” on appetite.
- Patients navigating stricter coverage or budget limits: Situations where formularies, step‑therapy rules, or savings cards make semaglutide the more realistic long‑term option, even if tirzepatide could deliver a few extra points of weight loss.
How to Decide: Tirzepatide vs. Semaglutide
Fit is never just about the molecule — it is how that drug lines up with your labs, comorbidities, side‑effect tolerance, schedule, and budget over several years.
In practice, that means some patients will start on semaglutide and stay there because it fully stabilizes their metabolic story, while others will escalate or switch to tirzepatide when the data — weight, A1c, liver markers, sleep, and cardiovascular risk — say they need more clinical firepower.
Which Compound to Use: Track, Talk, and Tweak
Which compound to use comes down to three moves: track, talk, and tweak. Tirzepatide’s dual‑action design gives it a higher ceiling for weight loss and A1c reduction in many patients, but the “better” drug is the one that fits your body, your risk, and your goals.
1. Track your goal
If you truly need 20%‑plus weight loss or aggressive multi‑system change (diabetes, MASLD, OSA, stacked CV risk), clinical data point toward starting the conversation with tirzepatide.
If your goals are strong but more modest — steady double‑digit loss and proven cardiovascular protection — semaglutide remains a heavyweight with the longest outcome track record.
2. Talk with a real clinical partner
Come to your visit ready to lay out your full story: diagnoses, meds, prior weight‑loss attempts, current energy and sleep, and the percentage of weight loss you actually need to get your life back.
3. Tweak the protocol on data
You start on the lowest effective dose, move up slowly, and watch weight, A1c, liver markers, sleep, and tolerability.
If semaglutide normalizes your numbers and you feel good, there is no rule that says you must “graduate” to tirzepatide. If your body is resistant or side effects get in the way, you have room to switch, adjust dose, or change agents.
Yunique Medical — We Don’t Wait for the Crash
Yunique Medical treats metabolic disease as a precision problem, not a prescription pad problem. Before a single dose of tirzepatide or semaglutide is ordered, you get a deep look at hormones, micronutrients, inflammation, liver health, insulin dynamics, and cardiovascular risk so the protocol is built around your actual biology, not an average trial patient.
Bring the fatigue, the “I’ve tried everything,” and the half‑finished injections in your fridge. The team builds a plan that uses modern agents like tirzepatide and semaglutide alongside targeted nutrition, resistance training, sleep work, and follow‑up labs — the details that turn a good response into a durable, life‑changing one.
Our Services
We offer a wide range of services to support your wellness journey, including:
- Hormone Optimization
- Infusion Therapy
- Weight Loss Programs
- Cellular & Functional Medicine
- Precision Longevity
- HeartFit Program
- Sexual Enhancement
- Peptide Therapy
- HOCATT Biohacking
Our Locations
You can find us here:
- Port Orange, FL
- Lady Lake, FL (formerly Fruitland Park Office)
- Ocala, FL
Ready to find out which protocol finally matches your metabolism, your risk, and your goals?
Book your Yunique Medical consult and bring your labs, your questions, and your real target.
